The modern healthcare environment is saturated with technology designed to enhance patient safety, such as monitors, ventilators, infusion pumps, nurse call systems, and environmental alarms. Yet this very abundance of safety systems has created an unintended hazard: alarm fatigue. The phenomenon occurs when clinicians are exposed to an overwhelming number of audible and visual alerts, many of which are false or non-actionable, leading to desensitization, delayed responses, or even complete disregard for alarms. The result is a paradoxical erosion of safety in the name of vigilance.
In critical-care areas, telemetry units, and surgical suites, hundreds of alarms can sound per patient per day. Michels et al. define alarm fatigue as “the sensory overload and desensitization that occurs when clinicians are exposed to an excessive number of alarms, many of which are clinically insignificant” [1]. This overexposure has measurable consequences. Studies have correlated alarm fatigue with missed critical events, increased response times, and elevated stress and burnout among healthcare staff [2].
The Anatomy of Alarm Fatigue
Alarm fatigue arises from the intersection of several factors: technical, human, and organizational. Default alarm parameters are often set conservatively by manufacturers, resulting in tight thresholds and frequent triggering. Motion artifacts, sensor disconnections, and benign physiological variations further inflate alarm counts. When every beep demands attention, yet few require action, staff experience the cognitive equivalent of background noise. Over time, their responsiveness diminishes.
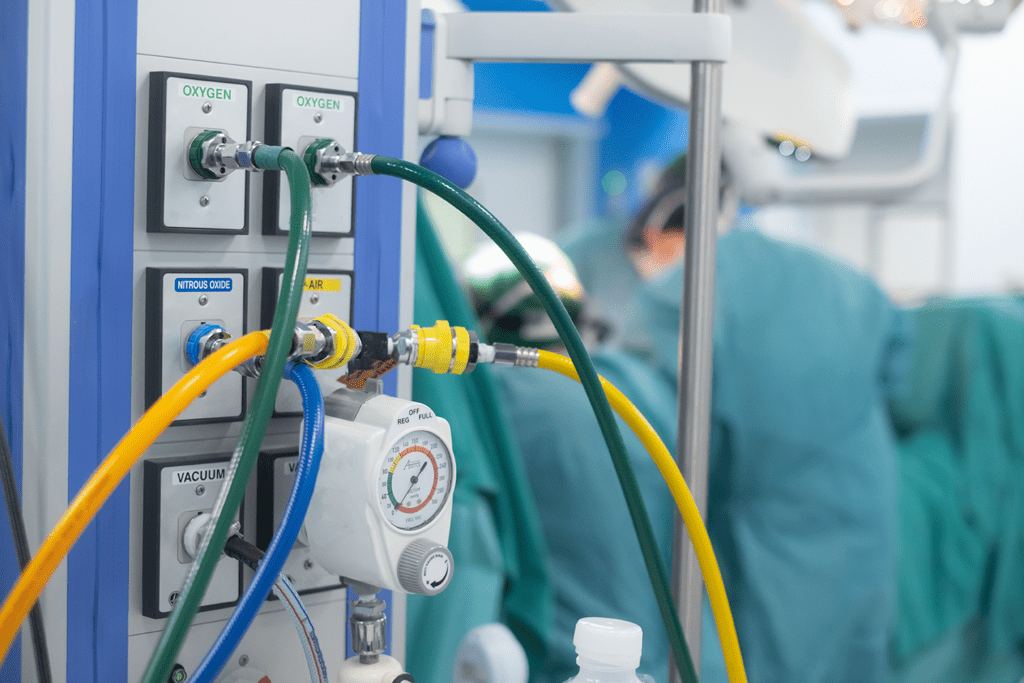
While physiologic monitors are the most visible sources, they are far from the only ones. The broader physical environment of care generates alarms from infusion pumps, bed-exit systems, ventilators, and environmental infrastructure such as medical gas sources, master, and area alarm panels. These panels, required under NFPA 99: Health Care Facilities Code, continuously monitor oxygen, nitrous oxide, medical air, vacuum, and other gases critical to patient life support. When improperly maintained or configured, medical-gas alarms can contribute to nuisance signals—low-pressure warnings during brief maintenance events or transient sensor fluctuations that mimic supply faults. The effect is cumulative: alarms from multiple subsystems, clinical and infrastructural, compete for attention, amplifying fatigue [3].
The Human and Organizational Dimension
Alarm fatigue is not simply a product of technology; it reflects the complexity of healthcare work. Clinicians interpret alarms within demanding workflows, balancing competing priorities and cognitive loads. Research has shown that when false-alarm rates exceed 85 percent, a common statistic in intensive-care environments, staff begin to subconsciously categorize alarms as “non-credible,” even when an occasional one signals true danger [4].
Emotional and physiological stress also compounds the issue. Continuous noise exposure elevates cortisol levels, contributes to fatigue and irritability, and has been associated with burnout and communication errors [5]. The auditory environment of a typical hospital, often exceeding recommended decibel levels, thus becomes both a safety and an occupational health concern.
Regulatory and Safety Perspectives
Recognizing the scope of the problem, The Joint Commission designated clinical alarm safety as a National Patient Safety Goal (NPSG.06.01.01) in 2014 [6]. Hospitals are required to inventory all alarm systems, identify critical alarms, and establish policies for parameter settings and response. Similarly, ECRI Institute has consistently listed alarm hazards among the “Top 10 Health Technology Hazards” for over a decade [7]. Both organizations emphasize a system-wide approach that includes understanding alarm sources, prioritizing actionable events, and tailoring alarm limits to the clinical context.
Integrating Infrastructure and Clinical Alarms
Efforts to reduce alarm fatigue often concentrate on patient-monitoring systems but overlook the role of facility-based alarms such as those tied to medical-gas manifolds, compressors, and vacuum pumps. These alarms are vital. A sudden drop in oxygen supply pressure or medical-air failure can precipitate life-threatening conditions across multiple patients simultaneously. Ensuring these alarms are clearly differentiated by tone, color, and annunciation from bedside alerts helps maintain their credibility.
Best practice calls for integrating medical-gas alarm data into centralized facility monitoring systems while maintaining distinct visual or auditory cues for infrastructure events. This approach aligns with NFPA 99 § 5.1.9.4, which requires distinct signal prioritization for master, area, and local source alarms. When such systems are properly configured, non-urgent technical alarms (e.g., maintenance conditions) can be logged without generating unnecessary bedside alerts, reducing cognitive clutter.
Evidence-Based Strategies for Mitigation
The literature supports several overlapping strategies to combat alarm fatigue. First, establish a multidisciplinary alarm management program that includes clinical, biomedical, and facilities personnel. This team should review alarm data trends, classify alarms by actionability, and adjust thresholds based on patient population and care setting [8].
Smart configuration, such as delaying annunciation for transient conditions, customizing thresholds, and avoiding redundant alarm pathways, has proven highly effective. In one neonatal ICU project, the number of alarms was reduced by more than 60 percent through targeted adjustments to monitor defaults and delay settings [9].
The “human factor” in alarm system design is a critical consideration. Standardizing alarm tones, using intuitive visual displays, and minimizing overlapping sounds across devices improves staff recognition and reduces response time. Alarm notifications should be graded by urgency, ensuring truly critical alarms (for example, a vacuum source failure) are unmissable but not accompanied by dozens of minor alerts [10].
Education and culture also play a pivotal role. Clinicians need training on the rationale behind alarm parameters, correct sensor application to minimize artifacts, and appropriate use of pause or silence features. Equally important is awareness of environmental alarms, including medical gas systems, so that staff understand which alerts require immediate action versus maintenance follow-up [11].
Finally, data analytics and emerging technologies offer new opportunities. Centralized alarm management software can track alarm frequency, categorize nuisance sources, and suggest parameter optimizations. Machine learning algorithms are being explored to cross-validate signals, combining physiological data with sensor quality indicators to suppress likely false alarms before they reach clinicians [12]. These innovations must, however, be implemented cautiously and validated in real-world settings.
Sustaining Improvement
Alarm management is not a one-time initiative but an ongoing process. Device upgrades, patient acuity changes, and staff turnover continually reshape the alarm environment. Institutions that sustain progress typically conduct periodic audits, publish unit-level alarm statistics, and celebrate teams that achieve meaningful reductions. Embedding alarm awareness into orientation, simulation training, and safety huddles reinforces a culture in which every alarm, clinical or infrastructural, remains credible.
Reframing the Narrative
Ultimately, alarm fatigue reflects a mismatch between system design and human attention. The goal should not be to silence alarms but to restore their meaning. By uniting biomedical engineering, nursing, and facilities management, healthcare organizations can transform a noisy, fragmented alert landscape into a coherent, prioritized, and human-centered safety network. Reducing alarm fatigue protects patients, supports caregivers, and strengthens the very systems designed to keep people alive.
References
- Michels, G., et al. Alarm Fatigue in Intensive Care Nursing: A Systematic Review. PLOS ONE, 2020. PMC7697990.
- Sendelbach, S., Funk, M. Alarm Fatigue: A Patient Safety Concern. AACN Advanced Critical Care, 2013.
- NFPA 99: Health Care Facilities Code. 2018 Edition.
- Cvach, M. Monitor Alarm Fatigue: An Integrative Review. Biomedical Instrumentation & Technology, 2012.
- Xie, H., Kang, J. The Impact of Noise on Staff Performance in Healthcare Environments. Journal of Environmental Psychology, 2021.
- The Joint Commission. National Patient Safety Goal 06.01.01: Clinical Alarm Safety. Updated 2024.
- ECRI Institute. Top 10 Health Technology Hazards. Annual Reports, 2014–2024.
- Funk, M., Clark, J. T. Managing Monitor Alarms in the Hospital: Strategies for Reducing Alarm Fatigue. Critical Care Nurse, 2020.
- Bonafide, C. P. et al. Reducing Alarm Frequency and Noise in a Pediatric Intensive Care Unit. Pediatrics, 2015.
- Block, F. E. Alarm Design for Clinical Environments. Anesthesia & Analgesia, 2019.
- Scott, L. A. Education Strategies to Reduce Alarm Fatigue in Nursing Practice. Journal of Nursing Care Quality, 2020.
- Hu, X. et al. Machine Learning for Reducing False Physiologic Alarms in Critical Care. IEEE Transactions on Biomedical Engineering, 2023.